 Ever wonder why vitamins go from A to E, then straight to K? It seems strange, but there’s a reason. It involves chickens.
Ever wonder why vitamins go from A to E, then straight to K? It seems strange, but there’s a reason. It involves chickens.
In 1929, a Danish nutritional scientist named Dr. Henrik Dam was studying the effects of cholesterol. During this study, he noticed that chickens who were put on a fat-free diet became ill and suffered from uncontrolled bleeding and bruising.
When the bleeding didn’t stop after restoring cholesterol to their diets, Dr. Dam realized that there must be another fat-soluble nutrient in their old diet that controlled blood clotting. With a bit of effort, he identified this nutrient and named it vitamin K, for koagulation (Danish for coagulation!)
Our understanding of vitamin K has flourished in the 90 years since Dr. Dam’s discovery. Today, we know that vitamin K isn’t just one vitamin, but a family of fat-soluble vitamins that share a similar molecular structure. And mounting clinical evidence over the past two decades has shown its role in human health goes well beyond blood clotting. Vitamin K (and in particular, vitamin K2) plays an essential role in cardiovascular and bone health. New research shows promising links to other health benefits like adolescent growth, blood sugar support, pregnancy, kidney health and even aging skin.
Despite all these advances in research, it is still one of the most misunderstood nutrients in medicine today.
We’ve put together this primer to clear up some common misconceptions of vitamin K. And we hope that by reading this, you’ll better understand what vitamin K is, appreciate what it can do for your body, know which forms to choose, and how to best use it for your continued good health.
Why does confusion about this vitamin linger to this day?
 Research on vitamin K persisted in the decade following Henrik Dam’s initial discovery in 1935. In the late 1930s, an American researcher named Edward Doisy succeeded in isolating vitamin K, isolating its molecular structure. This form later became known as vitamin K1.
Research on vitamin K persisted in the decade following Henrik Dam’s initial discovery in 1935. In the late 1930s, an American researcher named Edward Doisy succeeded in isolating vitamin K, isolating its molecular structure. This form later became known as vitamin K1.
In 1943, Dam and Doisy shared a Nobel Prize in medicine for their discovery of this “coagulation” vitamin. Unfortunately, this such recognition solidified many of the misunderstandings we see today.
You see, Dam, Doisy and other researchers at the time had already identified and characterized the structure of another micronutrient, vitamin K2. But it didn’t occur to them to treat K1 and K2 as separate micronutrients, with different benefits and unique properties. Instead, K1 and K2 were considered to be simply structural variants of the same vitamin, with the same biological role.
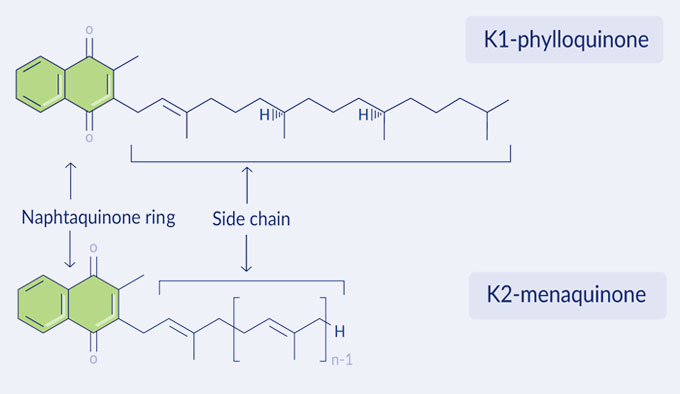
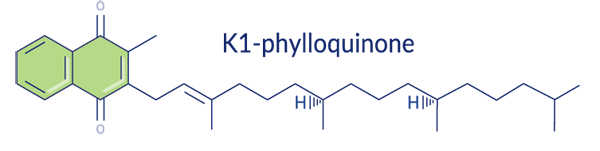
Looking at K1 and K2 side by side, you can imagine why Dam and Doisy thought they were variations of the same vitamin. All K vitamins have a naphthoquinone ring and a side chain of hydrogen and carbon atoms (called isoprenoids). Different forms of vitamin K have soprenoid side chains of different lengths and saturation. We’ll see later why these structural variations matter.
With the Nobel Prize, the fates of K1 and K2 became irrevocably intertwined for the next fifty years. All variations of vitamin K were only known for their role in blood clotting. A further corollary was established: All vitamin K deficiencies were rare and obvious, since it was assumed that a deficiency in vitamin K would result in some kind of bleeding disorder.
So final were these conclusions that little effort was spent to expand the body of vitamin K knowledge for the next thirty years. A big loss for vitamin K2, whose far greater role in the body was left undiscovered. Even worse, no one was looking for vitamin K2 deficiencies, which as we now know is quite widespread.
 At the same time Dam and Doisy were conducting their research, mild-mannered Dr. Weston Price, a Canadian with a small dental practice in Ohio, wondered why so many of his patients had terrible teeth. He hypothesized that there was something about the rapidly modernizing diet that was linked to declining dental health. Dr. Price sought out pre-industrial populations scattered across the globe in an effort to study this relationship between tooth decay and nutrition.
At the same time Dam and Doisy were conducting their research, mild-mannered Dr. Weston Price, a Canadian with a small dental practice in Ohio, wondered why so many of his patients had terrible teeth. He hypothesized that there was something about the rapidly modernizing diet that was linked to declining dental health. Dr. Price sought out pre-industrial populations scattered across the globe in an effort to study this relationship between tooth decay and nutrition.
In a series of perilous expeditions, he made his way to remote villages in the mountainous pockets of Switzerland, settlements along the rugged coasts of the Outer Hebrides, and the archipelagos of the South Pacific. He travelled with the nomadic Masai of Tanzania and the Nuer of the South Sudan, New Zealand Maori, the Inuit of Alaska and the tribes of the Peruvian Amazon and Andes. He observed that populations that maintained their traditional diet did not suffer from the tooth decay or malocclusion that was rampant back home. Instead, he found square jaws with neat, straight rows of teeth. When the same families were introduced to common processed foods, they would develop cavities and dental decay.
Armed with a camera, he would take photos of siblings – where the older child was
raised on a traditional indigenous diet and the younger living on imported foods. Where the first child would have well formed dental arches, the second would have many misaligned teeth.
 It was a predictable pattern, and in addition, Price noticed several other symptoms of declining health, such as slow healing bone fractures.
It was a predictable pattern, and in addition, Price noticed several other symptoms of declining health, such as slow healing bone fractures.
His fieldwork throughout the 1920s and 1930s yielded over 15,000 such stark photographs. When he returned, he detailed his ethnographic and nutritional studies in a book called Nutrition and Physical Degeneration. Without the benefit of our understanding of modern nutrition, Price hypothesized that these declines in dental health were not the result of some toxin in American diet, but the “absence of some essential factors”. He tested and analyzed thousands of samples of traditional foods for their nutritional content and compared them to common foods of the time. What he found was that many of the traditional foods, like fish eggs and the butterfat of grass-fed cows, were rich in fat-soluble nutrients.
He deduced that there was some activator or catalyst in the fat-rich diet that allowed the body to make use of other macronutrients like minerals. One activator had a significant affect on the health of bones and teeth, but since he could not identify or chemically isolate it, he labelled it as Activator X.
For years, physicians and nutritionists debated what this mystery Activator X could be. Some thought it might be a kind of essential fatty acid like EPA. Sixty years after Activator X was first mentioned, researchers now believe Activator X to be vitamin K2.
Vitamin K2 itself is not a single nutrient, but is itself a collection of molecules called menaquinones. These menaquinones share the same naphthoquinone ring as vitamin K1. However, while vitamin K1 has a monounsaturated side chain, menaquinones have unsaturated isoprenoid side chains of varying lengths.
A menaquinone with four isoprenoid units is called MK-4, five units MK-5 and so on up to MK-14. The two most common menaquinones identified for human health are MK-4 and MK-7.
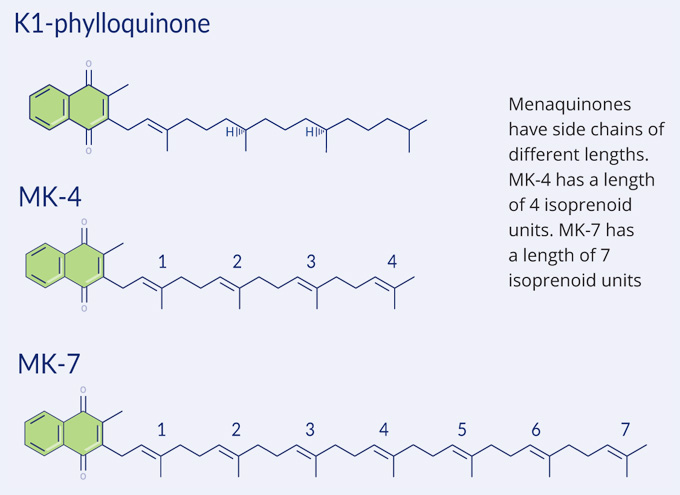
MK-4 and MK-7 have some functional differences. The lengths of the side chains help determine the lifespan in the body. MK-4 has a much shorter half-life in the body than MK-7, passing through the body in a matter of hours. MK-7, with its much longer side chain, has a half-life of three days.
MK-7, with its longer half-life, is also capable of reaching more parts of the body than MK-4. While MK-4 is good at supporting the soft tissues in the body, MK-7 is able to reach and support the liver and bone.
Learn about how vitamin K2 works, why it’s important, and how it can help you.


 The vitamin K family is discovered. Danish scientist Dr. Henrik Dam describes a fat-soluble factor that reduces bleeding in chicks fed an extremely low-fat diet. He names this factor vitamin K, for koagulation. A few years later, American biochemist Edward Doisy determines the chemical structure of vitamin K and succeeds in synthesizing it.
The vitamin K family is discovered. Danish scientist Dr. Henrik Dam describes a fat-soluble factor that reduces bleeding in chicks fed an extremely low-fat diet. He names this factor vitamin K, for koagulation. A few years later, American biochemist Edward Doisy determines the chemical structure of vitamin K and succeeds in synthesizing it. Dam and Doisy share the 1943 Nobel Prize in Medicine for their pioneering work on vitamin K1.
Dam and Doisy share the 1943 Nobel Prize in Medicine for their pioneering work on vitamin K1. Weston Price discovers ‘Activator X’ (K2) as a missing ingredient for tooth and bone health.
Weston Price discovers ‘Activator X’ (K2) as a missing ingredient for tooth and bone health. Vitamin K2 as MK-4 is approved as a drug in Japan.
Vitamin K2 as MK-4 is approved as a drug in Japan. Vitamin K2 is largely overlooked for a number of years before being rediscovered. Researchers in Japan begin to study the transfer of vitamin K2 between mothers and newborns.
Vitamin K2 is largely overlooked for a number of years before being rediscovered. Researchers in Japan begin to study the transfer of vitamin K2 between mothers and newborns. Studies investigate the relationship between K2, bone health and K2 biomarkers. During this time, researchers in Japan publish studies investigating the link between K2 and bone health. The impact of natto intake on bone stiffness and hip fractures is investigated.
Studies investigate the relationship between K2, bone health and K2 biomarkers. During this time, researchers in Japan publish studies investigating the link between K2 and bone health. The impact of natto intake on bone stiffness and hip fractures is investigated. Studies in 2015 demonstrate reductions in arterial stiffness and the slowing of arterial calcification, thereby reducing cardiovascular risk.
Studies in 2015 demonstrate reductions in arterial stiffness and the slowing of arterial calcification, thereby reducing cardiovascular risk.